Diagnosis for Hemophilia
I. FAMILIES
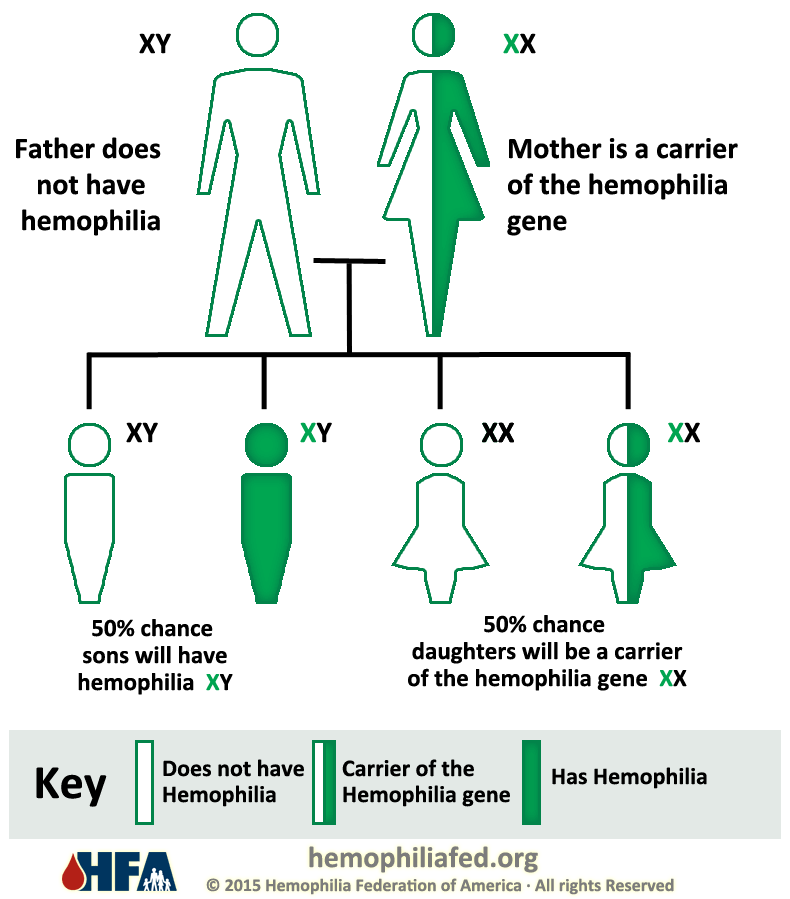
WITH A HISTORY OF HEMOPHILIA
If there is any family
history of bleeding disorder for instance bruises, surgery or unexplained
deaths among siblings or relatives should be considered and need to discuss with
doctor to confirm if hemophilia was the cause. Besides that, those individuals
who have or had family members with hemophilia will ask their baby boy to get
examined soon after birth because this disorder has higher possibility to occur
in males more than females. Not only that, in the best cases, testing for
hemophilia is planned before the baby’s delivery so that a sample can be drawn
from the umbilical cord blood immediately after birth. This sample will be
tested to predict the level of clotting factors. Apart from this, the umbilical
cord blood is better for testing hemophilia at determining low levels of factor
VII (8) than it is finding low levels of factor IX (9). This is because the
factor IX (9) levels will takes more time to develop and it is not at a normal
level until a baby’s age about 6 months.
II. FAMILIES
WITH NO PREVIOUS HISTORY OF HEMOPHILIA
About 33.33% of babies who are diagnosed with
hemophilia have no other family members with this type of disorder.
A doctor might do check up for hemophilia in a
newborn if:
- Unusual raised injuries (if a child is
not diagnosed with hemophilia during newborn period, the family might noticed
unusual bruising once the child started to crawl or stand).
- Bleeding in the scalp or brain after a difficult delivery or after using special devices to help deliver of infant.
- Bleeding goes on for a long period of
time after drawing blood as a sample and pricking the infant’s heel to draw
blood for neonates screening tests.
A. TESTS DURING PREGNANCY
1) AMNIOCENTESIS
§ Is
a medical procedure in which amniotic fluid is removed from the uterus for
testing and usually during weeks of 15 to 20 of pregnancy.
§ This
amniotic fluid contains the fetal cells and several types of chemicals produced
by the baby. 
2) CHORIONIC VILLUS SAMPLING (CVS)
§ Is
a medical procedure in which sample of chorionic villi is removed from the
placenta for testing usually during weeks of 10 and 13 of pregnancy.
§ The
sample can be taken through the cervix called as the transcervical or the abdominal wall called as the transabdominal.
B. SCREENING TESTS
1) COMPLETE BLOOD COUNT TEST
Ø The
most common test to measure the amount of hemoglobin, the number and size of erythrocytes
and the number of different types of leukocytes with platelets found
within blood plasma.
2) ACTIVATED PARTIAL THROMBOPLASTIN
TIME (APTT) TEST
Ø This
test helps to determine the ability for blood to clot.
Ø Examples
of clotting factors are Factors VII (8), IX (9), XI (11) and XII (12).
Ø The
blood clot may be affected by:
§ A
change in the activity of any of the clotting factors.
§ Low
levels of blood clotting factors.
§ The
absence of any of clotting factors.
§ Other
substances like inhibitors may affect the clotting factors.
§ An
increase in the use of the clotting factors.
3) CLOTTING FACTORS TESTS
Ø This
test is also known as factor assays which helps to predict the severity of Hemophilia.
SEVERITY
|
LEVELS
OF FACTOR VII (8) OR FACTOR IX (9)
|
NORMAL
|
50% TO 100%
|
MILD HEMOPHILIA
|
Greater
than 5% but less than 50%
|
MODERATE HEMOPHILIA
|
1%
to 5%
|
SEVERE HEMOPHILA
|
Less
than 1%
|










{kind=link}
{kind=link}
{kind=link}